Picking the right Molnlycke surgical gown sounds simple. Then you open a product catalog, pull up a budget spreadsheet, and check the infection control checklist — all at the same time. Suddenly, you’re trying to sort out whether BARRIER and PRIMARY are two different product lines or just the same gown with different names. Most procurement teams run into this. It’s more common than people say.
After going through EN 13795 compliance data, fluid resistance ratings, and real OR feedback, one thing stood out: there’s no single “better” gown. It’s a matching problem. The wrong pick doesn’t just drain the budget. It puts the sterile field at risk — and that’s a risk you can’t afford.
Here’s what matters when comparing these two series, broken down so the decision is clear.
The Confusion Starts Here: Why I Thought PRIMARY Was a Different Molnlycke Surgical Gown

Three product names. Three different formats. Zero indication they belong to the same line.
That’s what you run into researching Molnlycke surgical gowns across catalogs, distributor PDFs, and the official website at the same time. On one tab: “BARRIER® Surgical Gown Classic.” On another: “PRIMARY, standard performance.” On a third: “Molnlycke Primary Plus Surgical Gown” — with no “BARRIER” anywhere.
The conclusion feels obvious. Classic is one product line. Ultimate is another. PRIMARY looks like a third — something separate, maybe a budget-tier disposable surgical gown built to different standards.
It isn’t. They’re all BARRIER.
Here’s where the naming structure breaks down:
Official PDFs lead with “BARRIER® Surgical Gown Classic” in large headers
The Molnlycke website URL reads
/primary-standard-performance— No BARRIER branding visible at the page levelDistributor listings drop “BARRIER” and show ” Molnlycke Primary Plus Surgical Gown ” with nothing else
BARRIER also appears on isolation gowns on platforms like MedicalExpo. That makes the label feel like a loose, catch-all brand — not a focused surgical gown line
The product language adds to the confusion. PRIMARY pages say “standard performance” and “low- to moderate-risk surgical procedures.” Ultimate documentation pushes “high protection and high comfort.” Classic sits in the middle — described through technical specs, not a clear tier label.
There’s no single comparison table mapping PRIMARY, Classic, and Ultimate against EN 13795 or AAMI PB70 benchmarks. So the full structure stays hidden.
The fix: treat BARRIER as the umbrella brand. PRIMARY, PRIMARY Plus, Classic, and Ultimate are performance tiers within it — not separate competing lines. Get that hierarchy straight first. Then the real comparison between BARRIER and PRIMARY becomes a simple question: what protection level does the procedure need?
That’s where the actual decision starts.
My Honest Take on BARRIER PRIMARY: A Lightweight Surgical Gown for Low-Risk Procedures

BARRIER PRIMARY doesn’t try to be everything. That restraint is what makes it useful.
Cut through the branding and here’s what you get: a lightweight, single-use surgical gown built for one specific job. It protects the surgeon and patient during low- to moderate-risk procedures where fluid exposure is limited and case duration stays under 90 minutes. Tonsillectomies. Minor arthroscopies. Short laparoscopic cases. Excisional biopsies. These are procedures where a heavy, reinforced gown would be overkill — and expensive overkill at that.
What the Fabric Feels Like
The material is SMS nonwoven polypropylene — spunbond-meltblown-spunbond construction — in the 25–45 gsm range. That weight matters more than it sounds.
At that gsm, the gown drapes like soft paper. Not crinkled plastic. No stiff panels. No PE-film overlay crackling with every movement. Clinicians who switch from reinforced gowns to an SMS-only disposable surgical gown at this level often report a 30–50% drop in movement noise. That’s a small thing. Over a three-hour shift, it adds up.
Breathability follows the same logic. SMS fabrics at this weight deliver air permeability around 20–60 L/m²/s and moisture vapor transmission in the 500–1,500 g/m²/24 h range. Compare that to fully laminated high-barrier gowns. Those often fall below 500 g/m²/24 h. You’ll feel the difference inside a warm OR after the first hour.
Where the Barrier Protection Lands
BARRIER PRIMARY meets AAMI Level 2 performance under AAMI/ANSI PB70. Some configurations reach low Level 3:
Test | Level 2 Benchmark | Level 3 Benchmark |
|---|---|---|
Impact penetration (AATCC 42) | ≤ 1.0 g | ≤ 1.0 g |
Hydrostatic pressure (AATCC 127) | ≥ 50 cm H₂O | ≥ 50–100 cm H₂O |
Fluid exposure profile | Low | Moderate |
EU procurement teams should note the equivalent rating is EN 13795 Standard Performance — not High Performance. That’s not a weakness. It’s a spec match. The procedures PRIMARY targets don’t generate fluid volumes that need Level 4 protection.
The critical zones — front chest and sleeves — meet the declared barrier thresholds. Non-critical areas like the back use lighter fabric. This keeps total gown weight down without weakening the zones that face real exposure risk.
The Three Questions That Lead You Here
Before defaulting to a higher-level reinforced surgical gown , ask yourself three things:
How much fluid do I expect?
How long will the procedure run?
What’s my role — primary surgeon, assistant, or observer?
For short, low-fluid cases, those three answers point toward a lightweight fluid-resistant surgical gown at Level 1–2. PRIMARY fits that decision logic well.
What it doesn’t fit: open cardiovascular surgery, major trauma, cesarean sections, or any case where strike-through risk is real. Those procedures need AAMI Level 4 barrier protection — and that’s where the BARRIER Ultimate series takes over.
PRIMARY Is Not Enough: High-Risk Surgeries Need a High Barrier Surgical Gown

The number that changed my thinking was 9 liters.
That’s the upper end of irrigation fluid used in a single hip replacement — pulsatile lavage alone, before you count blood loss. At that volume, the question stops being “is this gown comfortable?” and becomes “will this gown still hold?”
BARRIER PRIMARY won’t hold. Not across 90 to 180 minutes of direct splash exposure to the chest, shoulders, and sleeve seams of the primary surgeon. That’s not a criticism — it’s a specification. PRIMARY targets AAMI Level 2 conditions. Joint replacement surgery runs at Level 3, pushing Level 4. Those two realities don’t overlap.
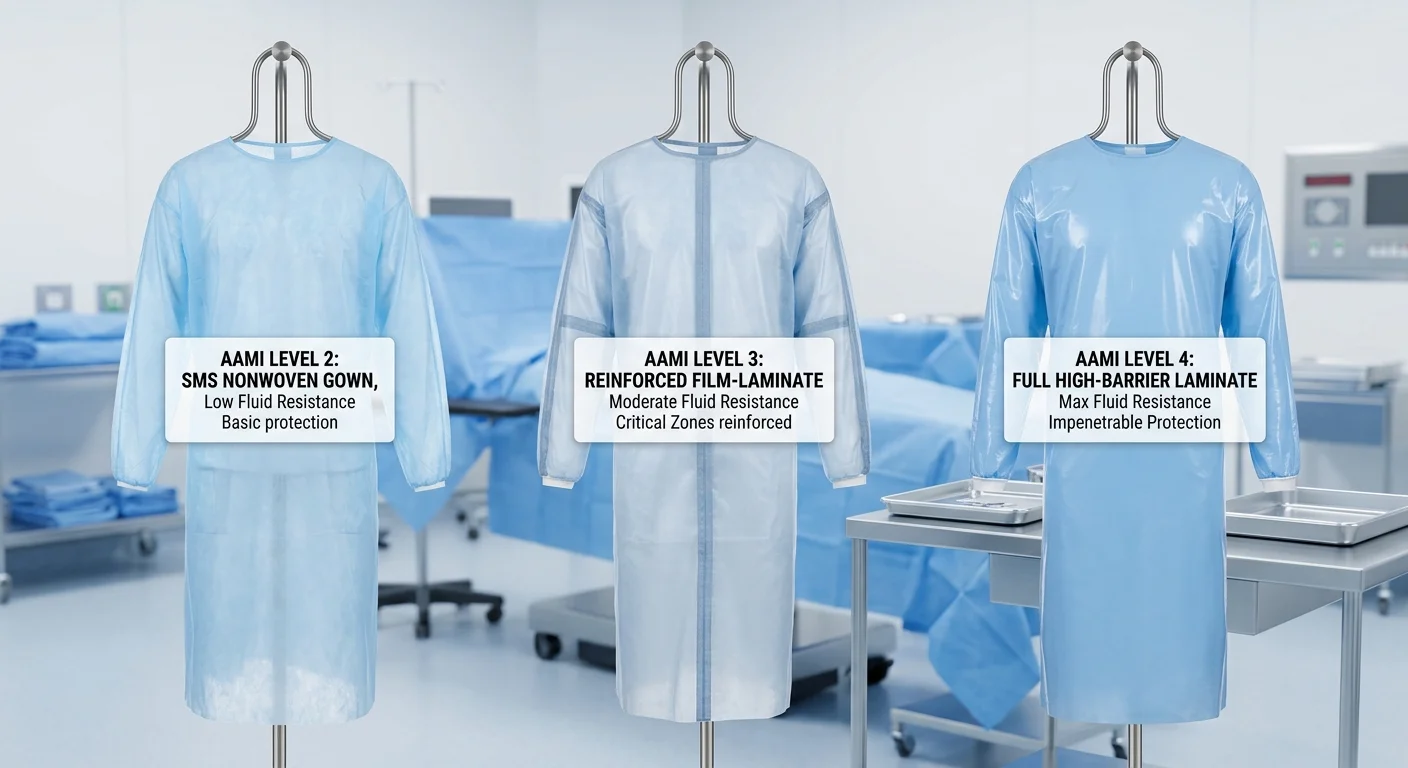
What AAMI Levels Measure in the OR?
AAMI’s four-tier classification is concrete, not abstract. Each level centers on three variables: type of fluid, volume of exposure, and duration of contact. Push any one of those variables higher, and your required protection level goes up with it.
Here’s where PRIMARY’s Level 2 ceiling becomes a problem in real procedures:
Procedure | Fluid Volume | Duration | Indicated Level |
|---|---|---|---|
Tonsillectomy / minor arthroscopy | Low | < 60 min | Level 1–2 ✓ PRIMARY |
Mastectomy / open GI procedure | Moderate | 60–120 min | Level 3 |
TKA/THA (joint replacement) | 3–9 L irrigation + 500–1,500 mL blood | 90–180 min | Level 3–4 |
Trauma laparotomy | > 1,000–2,000 mL blood + irrigation | Variable | Level 4 |
Open cardiovascular / thoracic | 500–2,000+ mL, aerosolized droplets | 3–6 hours | Level 4 |
Cesarean section | Moderate-to-high blood + amniotic fluid | 45–90 min | Level 4 |
Level 2 gowns are tested for mild spray, brief contact, and minimal hydrostatic pressure.
Trauma and cardiovascular procedures produce something different: arterial spurting, sustained pressure against sleeve seams, micro-droplet aerosolization from bypass circuits — across hours of continuous wear.
These are not edge cases. They are standard OR conditions for a large share of hospital surgical volume.
Where PRIMARY Fails Under High-Fluid Load?
The failure isn’t dramatic. That’s exactly the problem.
Strike-through on a Level 2 SMS surgical gown under high hydrostatic pressure is gradual. Fluid wicks through stitched seams. Saturation builds at the forearm cuff junction. Slow penetration follows through the chest panel after prolonged contact. By the time you see it, the sterile surgical gown has already been compromised.
High-barrier reinforced surgical gowns at Level 3–4 use a different construction approach:
Multi-layer nonwoven laminates in critical zones — not single-layer SMS
Sealed seams across the front torso and sleeve areas — stitched seams wick fluid; sealed seams block it
ASTM F1671 viral penetration resistance in Level 4 critical zones — a test PRIMARY is never required to pass
Reinforced front panels and forearm sections built to hold barrier integrity under mechanical stress from retractors, power tools, and orthopaedic instruments
Open cardiovascular surgery is a clear example. The threat isn’t one high-pressure splash. It’s hours of sustained hydrostatic pressure from direct contact with blood and priming solutions. Level 4 surgical gown barrier protection is the standard validated for that combination of duration and fluid load. A disposable surgical gown rated at Level 2 is built for a blood draw — not a six-hour bypass procedure.
The Decision That Protects Your Staff
The cost gap between a Level 2 and a Level 4 sterile surgical gown is real but small. What you’re weighing it against carries more weight: occupational fluid exposure, post-exposure testing and prophylaxis, surgical site infection risk from fluid wicking back toward the operative field, and the staff anxiety that comes with any strike-through event.
Before each high-risk case, three questions set your minimum standard:
Expected fluid volume — irrigation above 2–3 L or blood loss above 500 mL puts Level 2 under-spec
Procedure duration — anything beyond 90 minutes puts sustained hydrostatic pressure on SMS-only construction
Role and proximity — a primary surgeon with hands inside a pelvic or thoracic cavity needs Level 4; a scrub nurse at a distance may need Level 3
Cross any one of those thresholds, and BARRIER PRIMARY is the wrong gown for that procedure. Not because it fails any marketing standard — it doesn’t. It was never built for those conditions.
That’s the line that matters for OR gown infection control: not which gown is better overall. Which one matches the actual fluid load, duration, and role in the case you’re about to run?
The High-BARRIER Molnlycke Surgical Gowns I Put on the Shortlist
Three gowns. Three different answers to the same question: how much fluid is too much?
That’s the lens I kept coming back to. Not which gown looked best on a spec sheet — but which one held up when fluid volume, case duration, and exposure risk were all weighed together.
Here’s what made the shortlist, and why each one earned its place.
BARRIER® Classic SP — The Breathable Floor
The Classic SP uses spunlace nonwoven — a pulp-and-polyester hydroentangled fabric. It moves and breathes in ways film-reinforced gowns can’t match. Air permeability sits in the 10–20 cm³/cm²/s range. WVTR runs near 4,000–7,000 g/m²/24h. For a long, low-to-moderate activity case, those numbers matter.
What it won’t do: hold under pressure.
Its EN 13795 Standard Performance / AAMI Level 2 rating validates it for synthetic blood penetration at 2 psi (≈13.8 kPa). Go beyond that — sustained splash, high irrigation volume, prolonged contact — and this gown was never built for those conditions.
Think of it as the right ceiling for moderate-exposure cases. It’s not the starting point for wet surgery.
BARRIER® Classic High Performance — The One That Held
This gown changed the comparison for me.
EN 13795-1 High Performance. AAMI Level 3. Validated at 3.5 psi (~24 kPa) synthetic blood pressure. The reinforced front panel and sleeves use a film or membrane layer — liquid-proof in critical zones, not just repellent. Non-critical zones stay spunlace, so you keep some breathability where it counts.
The trade-off is real and measurable:
WVTR in reinforced zones drops to 800–1,500 g/m²/24h
Surgeons in procedures past two hours report +1–2°C local skin temperature in those zones
That’s worth knowing upfront. For orthopaedics, urology with irrigation, or major trauma — cases with sustained, high-pressure fluid exposure — the construction logic holds up well.
Packaging comes in three layers. Sterile presentation stays intact from distribution to the scrub nurse. FSC-certified paper components are used where applicable.
BARRIER® Ultimate — For Cases Where Level 3 Falls Short
The Ultimate line covers the far end of the protection range: AAMI Level 3–4 territory. It pairs advanced spunlace with a high-barrier laminate across the full front and sleeve surface. This surgical gown covers cases where viral penetration resistance (ASTM F1671) is a factor, not just blood and irrigation volume.
Breathability in reinforced zones drops to near-zero air permeability. That’s the direct cost of full fluid protection over hours of exposure. For open cardiovascular surgery or major trauma laparotomy, that trade-off makes clinical sense. For shorter or drier cases, you’re carrying thermal burden with no real return.
What the Three Tiers Tell You
Gown | Classification | Barrier Mechanism | Best Fit |
|---|---|---|---|
BARRIER® Classic SP | EN 13795 Standard / AAMI L2 | Fluid-repellent spunlace | Moderate-duration, low-to-moderate splash |
BARRIER® Classic HP | EN 13795 High Performance / AAMI L3 | Film-reinforced critical zones | Wet surgery: ortho, trauma, urology |
BARRIER® Ultimate | AAMI L3–L4 (estimated) | Full-coverage high-barrier laminate | High-volume fluid + viral exposure risk |
The right gown isn’t the most protective one on the list. It’s the one that fits the pressure, duration, and fluid volume of the case you’re running, with the least breathability sacrifice you can justify clinically.
That’s where the real decision sits.
A Simple Way to Choose a Molnlycke Surgical Gown Based on Fluid Risk
Two questions. That’s all this decision takes.
Every other variable — material weight, breathability ratings, packaging format — follows from the answers to these two:
Is the fluid risk for this procedure low-to-moderate or high?
Does this case require viral barrier protection (AAMI Level 4)?
Answer those two correctly, and the right Molnlycke surgical gown becomes obvious.
How to Measure Fluid Risk in Practical Terms
Fluid risk isn’t abstract. Three measurable factors define it:
Expected fluid volume. Irrigation or blood loss below 500–1,000 mL with a dry field puts you in low-to-moderate territory. Volume above 1,000 mL is a clear signal. So is a surgeon whose chest and sleeves are soaked more than once. Either of those pushes the case into high fluid risk.
Procedure duration. For under two hours, the cases stay low-to-moderate. Past two to three hours of open surgery, hydrostatic pressure builds against the gown fabric — splash frequency aside. Default to high fluid risk for any long open procedure.
Surgical category. Certain procedure types fall into the same tier every time:
Risk Level | Typical Procedures | Indicated AAMI Level |
|---|---|---|
Low | Excisional biopsy, tonsillectomy, adenoidectomy | Level 1–2 |
Moderate | Mastectomy, arthroscopy, open GI/GU (moderate blood loss) | Level 3 |
High | Open cardiovascular, trauma, laparotomy, C-section, open colectomy | Level 4 |
The Viral Barrier Question Changes Everything
A Level 3 reinforced surgical gown handles moderate fluid volume well. It does not pass ASTM F1671 viral penetration testing — because that was never its requirement.
Level 4 is the one AAMI classification that requires Phi-X174 bacteriophage penetration resistance. That’s the standard proxy test for bloodborne viral transmission. Any of these conditions means Level 4 — no exceptions:
Patient has confirmed or suspected bloodborne virus (HBV, HCV, HIV)
The procedure involves repeated deep cavity exposure with high-volume fluid
Institutional protocol requires Level 4 for open thoracic or trauma cases
The 3-Step Selection Path
Step 1 — Flag high fluid risk. Mark it high if any one of these applies: expected blood or irrigation ≥ 1 L, open procedure running ≥ 2–3 hours, or repeated soaking of the front torso and sleeves.
Step 2 — Ask the viral barrier question. A “yes” to any condition above sends you straight to a Molnlycke AAMI Level 4 sterile surgical gown.
Step 3 — Match the remaining cases by fluid tier:
Minimal exposure, short duration → Level 1–2 (BARRIER PRIMARY fits here)
Moderate fluid, 1–3 hours, no viral risk → Level 3
High fluid or viral risk → Level 4 , full stop
Four quick examples put this into practice:
Open colectomy — 2–3 hours, 1–2 L fluid, unknown hepatitis status → Level 4
Laparoscopic cholecystectomy — under 90 minutes, moderate irrigation, no viral flag → Level 3
Subcutaneous lump excision — 20 minutes, minimal bleeding → Level 1 or 2
Cesarean section — amniotic fluid plus blood, high soaking exposure → Level 4
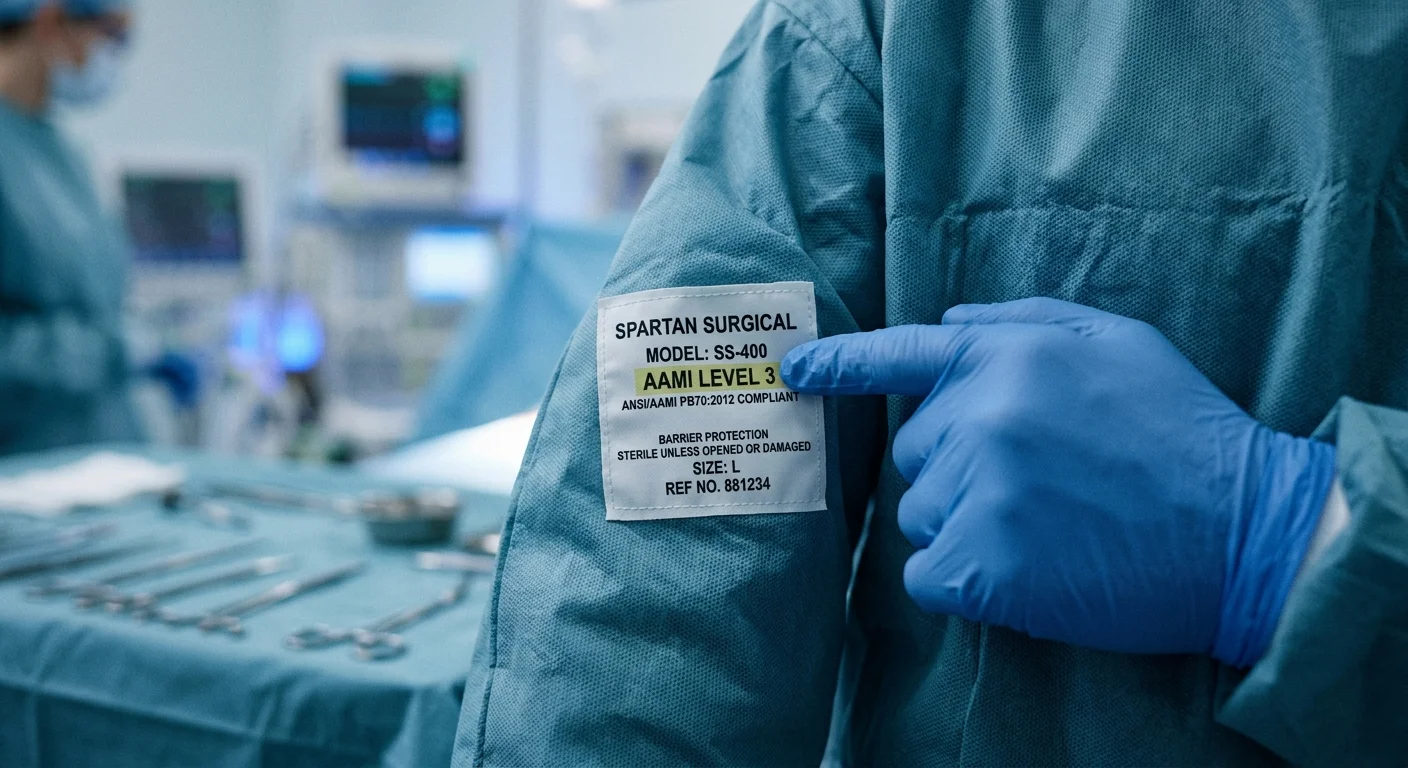
One packaging note worth keeping in mind: check that the “AAMI Level X” designation is printed on the Molnlycke label itself before accepting a distributor’s verbal claim. That label is your reliable verification point — nothing else is.
Three Questions I Wish I Had Asked Before Ordering Molnlycke Surgical Gowns
The purchase order was already submitted. Then the doubt arrived — quiet, persistent. The kind that settles in after a decision, not before it.
Three questions. That’s the gap between a well-matched gown order and an expensive mistake. Not three pages of compliance review. Not a committee meeting. Three questions the AAMI framework has always implied, but no one made explicit before the contract was signed.
Question 1: How much fluid do we expect — and for how long?
This isn’t rhetorical. AAMI PB70 builds its entire four-level classification on two variables: fluid volume and exposure duration. Before ordering, map your top 20–30 procedures by case count. For each one, name the fluid category — minimal, low, moderate, or high — and the typical case length.
The results tend to surprise people. In many acute-care ORs, only 10–25% of annual cases require Level 4 protection. The rest fall at Level 2 or 3. Defaulting everything to Level 4 — because it feels safer — doesn’t change that number. It changes the invoice.
Question 2: What is each person’s role in the procedure?
A primary surgeon working inside a pelvic cavity for three hours faces a very different fluid risk than the circulating nurse charting across the room. AAMI’s framework accounts for this difference. Procurement teams often miss it.
A mixed-level stocking strategy makes sense here. Use Level 3 or 4 for scrubbed primary roles. Use Level 1 or 2 for circulators and observers. This approach cuts total gown spend without lowering the protection standard for anyone in the field.
Question 3: Did we validate material performance beyond the AAMI label?
The AAMI level is necessary. It isn’t enough on its own.
Before committing to a bulk Molnlycke surgical gown order, ask your clinical rep for three specific data points:
MVTR (moisture vapor transmission rate) — get this for both critical-zone panels and non-critical back panels
GSM of the fabric — heavier nonwovens carry higher barrier ratings, but they also trap more heat across a four-hour open case
Lint and flammability data — this matters for implant services, ophthalmic cases, and any OR using electrocautery in oxygen-enriched conditions
Most teams skip one practical step: trial at least two Molnlycke gown lines within the same AAMI level. Collect structured feedback from 10–20 OR staff. Rate each gown on noise, heat retention, and comfort before locking in the annual SKU. A gown that passes every barrier benchmark but draws constant complaints about rustling or heat creates real operational problems over time.
The term “impervious” on a gown package means nothing specific. The AAMI level printed on the Molnlycke label is the one number with a standardized, validated meaning. Everything else is marketing language — and marketing language doesn’t hold up in a fluid-intensive open case.
Conclusion
Choosing between Molnlycke’s BARRIER and PRIMARY isn’t a product debate. It’s a patient safety decision wrapped in a procurement question.
Here’s what this comparison comes down to: PRIMARY earns its place in low-fluid, routine procedures where breathability and cost efficiency matter. But as fluid exposure risk climbs — orthopedic, cardiovascular, trauma — a reinforced surgical gown with verified AAMI Level 3 or EN 13795 high-performance classification is no longer optional. It’s the baseline.
The most expensive mistake an OR team makes isn’t over-specifying protection. It’s under-specifying it once.
Before your next order, run your surgical schedule against the fluid-risk framework covered here. Match the procedure, not the price tag.
Still weighing which Molnlycke surgical gown configuration fits your facility’s volume and case mix? The product comparison table above is your fastest route to a clear, data-backed decision.
Choose with intent. Your OR team — and your patients — deserve that.




